
Organ donation in Fortis Chennai
Background:
Organ donation after brain death has benefited some of the Indians. Vast majority still succumb to sequel of organ failure. The list of people in need of life saving organ transplant is growing. Our country has shortage of organ donors.Consent of family members is vital in increasing organ donors. We analysed our data to identify hindrances to organ donation.
Introduction:
In India there are over 100,000 people in need of life saving organ transplant. Major chunk of these people need either kidney or liver transplant. Annually, less than a third of them are transplanted, either with live donor or cadaver donor organ. Majority of them die because of lack of an organ.
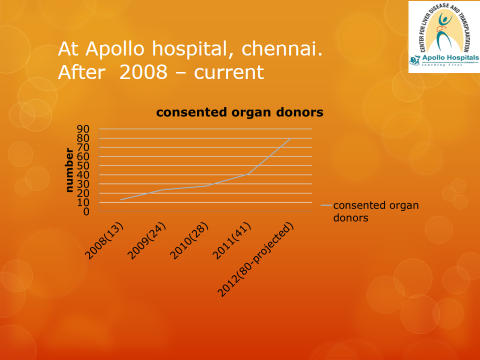
India has had organ transplantation act in place since 1994. The act legally accepted brain death as death itself. However it was not implemented on ground. Tamil Nadu government took a lead in this regard and further clarified and re-interpreted the central government rules, making it clear and easy for the physicians to declare brain death and paved way for cadaveric organ donation. Prior to 2007, the families who were aware and interested donated the organs of their family members which were only a hand full. Since then awareness has increased, and major private and public hospitals of south India have taken an initiative to promote organ donation and we have seen surge in cadaver organ transplantation. It is a good start, but we still have a long way to go. At Fortis hospitals, Chennai we have performed over 200 cadaver donor liver transplants in the last 5 years, which makes it the largest cadaver organ transplant centre in India. It has been an uphill struggle to promote organ donation.
Materials and methods:
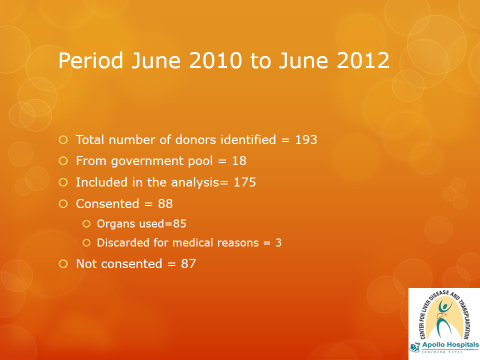
We prospectively collected the data between June 2010 to June 2012, from all the brain dead donors who were approached for organ donation at Fortis hospitals, Chennai, India. A dedicated team of highly motivated ICU nurses and social workers rounded in all our ICUs and followed patients with GCS of <4. Families of patients who progressed to brain death were approached for organ donation. This was done in consultation with hospital authorities as well as primary physician in charge of the patient. They recorded all the problems encountered in the process. For the purpose of the study 'family' meant wife/husband and any other first degree relative. And the 'extended family' meant those who accompanied the patient but were not part of 'family' as said above.
The primary outcome for our study was family consent to organ donation. Families who declined organ donation were asked to give the primary reason for declining consent. When no direct answer was not available, our co-ordinators recorded their opinion for declining consent. Potential organ donor families who declined organ donation (decline group) were compared with potential organ donor families who consented to donation (consent group). The decline and consent groups were compared test. Values are reported as mean standard deviation or raw percentages, and statistical significance was set at p < 0.05. The local Institutional Review Board approved this study.
Results:
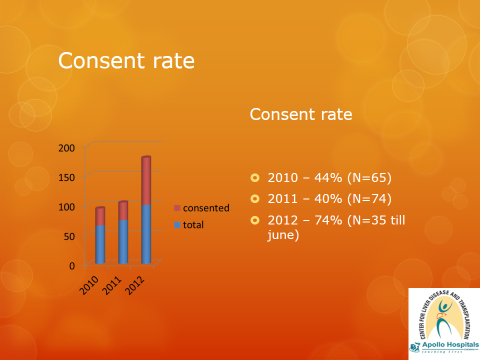
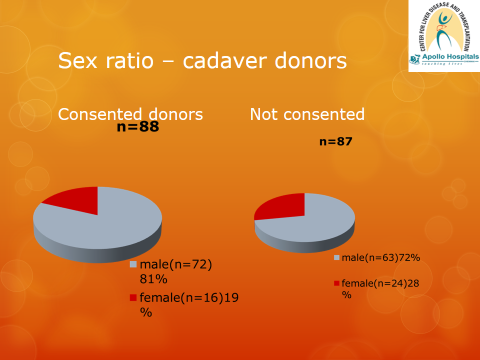
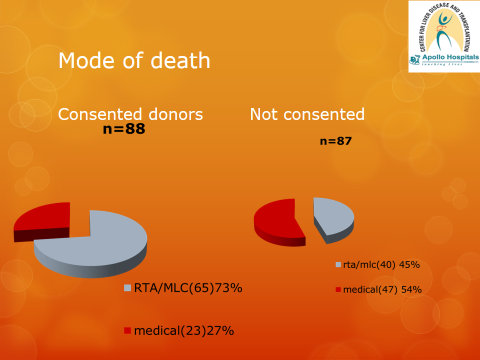
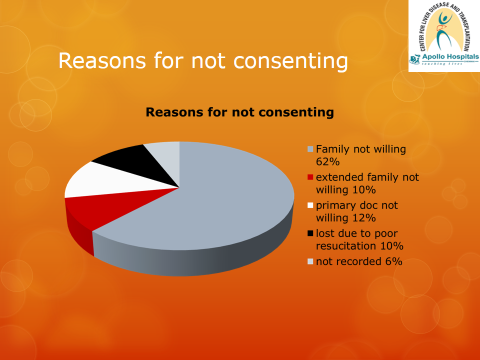
In this period a total of 175 donors were identified. Majority of the patients were males (77%), victims of road traffic accidents (59%). There was only one paediatric donor in this period. Overall consent rate was just over 50%. Among those who consented, over75% were victims of road traffic accidents. Those who died from medical causes were unlikely to consent (p, .005). The reasons for not consenting are listed in table 1.
Table 1
- Family not willing = 62% (54)
- Immediate Family willing but other members not willing= 10%(9)
- Primary doctor not allowing to approach family = 12%(11)
- Very unstable/poorly managed = 10%(9)
- (Arrested prior to brain death declaration)
- not recorded =6%( 4)
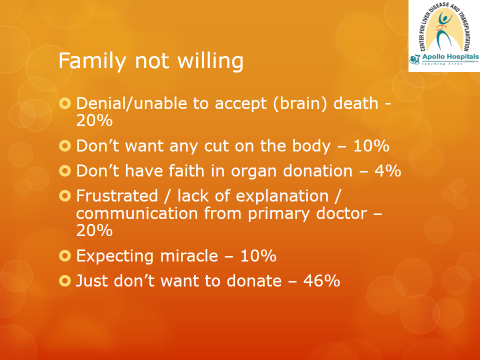
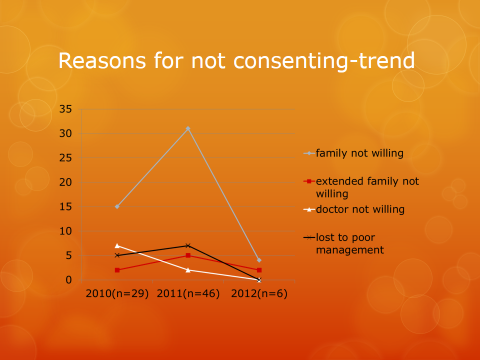
In about 12% of patients there was enormous amount of resistance by the primary physician for approaching the family which lead to loss of the donor. In the not consent group, Family just not willing to donate formed major chunk. Other reasons for not willing to donate were, inability to accept the concept of brain death(20%), they felt frustrated as adequate time/explanation was not given to them by the treating physician(20%), a few of the families did not want cut on the body (10%), some of them were expecting a miracle as their religious head had told them to pray and not donate organs(10%), minority of the patients said that they don't have faith in organ donation system.
Discussion
Our centre has been performing liver transplants since 2007. We have performed over 200 cadaver donor liver transplants and over 50 living donor liver transplants. Tamil Nadu has taken the lead in promoting and facilitating cadaver organ donation. As a result, over 90% of donations that happen nationally are from this state alone. Our hospital contributes about 50% of the donors to this program. This is possible because of the vision and forward thinking nature of the administrators and co-operation from our nursing, medical and other personnel.
Thanks to the media, awareness of organ donation is on the rise. We have seen surge in organ donation form places in Tamil Nadu like Coimbatore, Madurai, Salem and Trichi. On many instances, family had come forward to donate organs of the deceased family member. The doctors had not even mentioned organ donation to these families. As a policy they did not actively encourage organ donation.
Initial struggle
Even in the best of the centres, brain dead patients' families areneither counselled adequately nor are given an option of organ donation. This is mainly because of misconceived ideas by the treating physicians. In this study, in about 12% of the cases, there was strong resistance by the treating physician. Co-ordinators were not allowed to approach the family. In the inception of our program, the resistance was even more. With appropriate education it has come down substantially, but we still face it regularly.
Educating the educated
Death of patient under a physician's care is perceived as failure of treatment. We all know that medical science cannot save every one. We all have our limitations. The usual tendency is to think, “If I say the patient died in spite of our treatment, what will the family think of me? will I get a bad name?”. It is easy to say “ patient is critical, we are doing our best” and thus avoid difficult situation of explaining concept of brain death.
When families face hopeless situation, most of them turn to religion for comfort or re-assurance. We have seen a few religious heads, very strongly re-assuring families and urging them to pray and that the patient will live!. On one occasion, priest said “I will resurrect the patient just like Jesus and he will come back to life”.The support that they get from astrologers and religious heads cannot be under estimated. But they must be realistic and refrain from giving false hopes to the grieving family and cheat others who are waiting for an organ of gift of life.
In certain situations, death is certain and we will not be able to alter the nature. In such a situation, it will be magnanimous to accept brain death and promote organ donation. One will be able to change 'death' into 'a gift of life'. In spite of all our best efforts, when life ceases in one, one must take it in the right perspective and when there is a chance, it must be passed on.
Role of co-ordinators/grief counsellors
We have very enthusiastic and highly dedicated co-ordinators and social workers. They play multifunctional role. They round in ICUs and follow patients with deteriorating GCS and those with GCS <5. Once all the brainstem reflexes disappear, with the help of critical care doctors and consent from the primary physician donor protocol is initiated, which is intravenous methyl prednisone and levothyroxine, ensure the patient has central line and arterial line for hemodynamic monitoring. In the appropriate clinical setting, brain death declaration is done as per the recommendations given by the Tamil Nadu go………..After the first declaration, the family is approached for organ donation at the right time.
The co-ordinators take away the conflict of interest present in the critical care doctor as well as the primary physician. Every brain dead patient's family is given a chance to donate organs. They also update family about the critical nature of the patient and brief them about the ongoing medical care. They develop rapport with the family and give them shoulder to cry on. They fill the void left by busy treating doctors. They work towards making this very difficult time to be as smooth as possible.
Higher consent rate among accident victims
The law in Tamil Nadu has made it mandatory for all private and public organ retrieving centres to perform post mortem examination (when necessary and by appropriate authority) after organ retrieval at the local hospital. This avoids delay in shifting the body to mortuary and waiting for post mortem examination to be done by the forensic expert. This benefit is offered to all Medico legal / road traffic accident victims. Perhaps, to avoid legal hassles associated with post mortem and to avoid associated delay in performing last rites, we see higher consent rate among MLC patients.
Male predominance among donors
Majority of our road traffic accident victims were riding two wheelers without helmets. Most of the lethal accidents happened in the city limits and not on the highway. Hit and run as well as 'slip and fall' were seen with equal frequency. We see male predominance among road traffic victims. It reflects male dominant working society. The consent rate among female victims of RTA was less. Looking at it from another angle, when males are the victims, women took decision to donate organs and vice versa. For such a striking contrast, we can only speculate, women are more sympathetic towards organ donation or the males express their desire to donate organs after their death(while women don't) or women are good at taking day today decisions!
Summary
There is wide gap between demand for organ donors and recipients which needs to be bridged. Promoting cadaveric organ donation can bring down illegal organ trading. Hospitals need to have active policy of promoting organ donation. One has to look beyond personal gain and work towards a better society. As a corollary to our study, make helmets compulsory for all those who ride on two wheelers. It saves lives.